
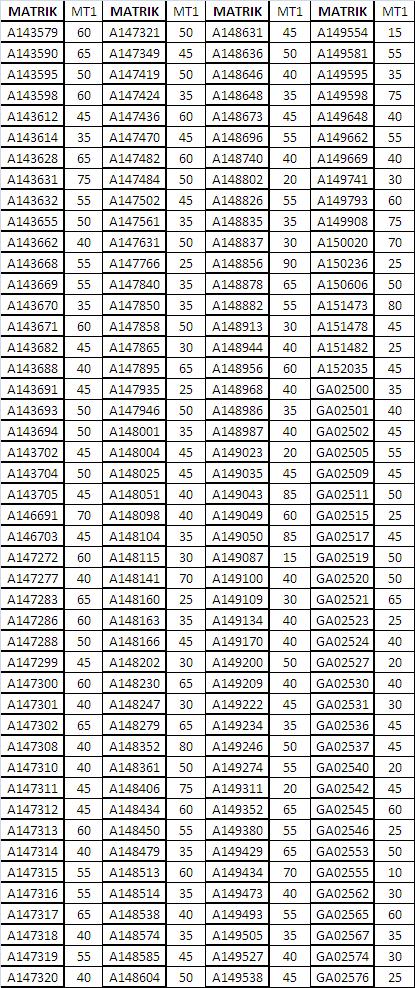
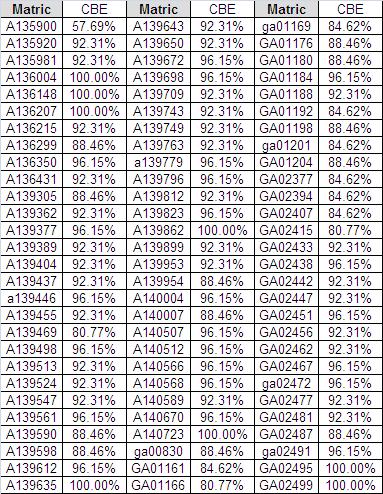
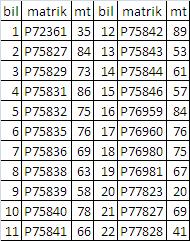
Individual Results
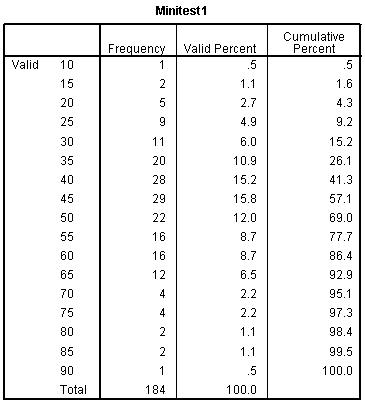
57.1% failed minitest 1
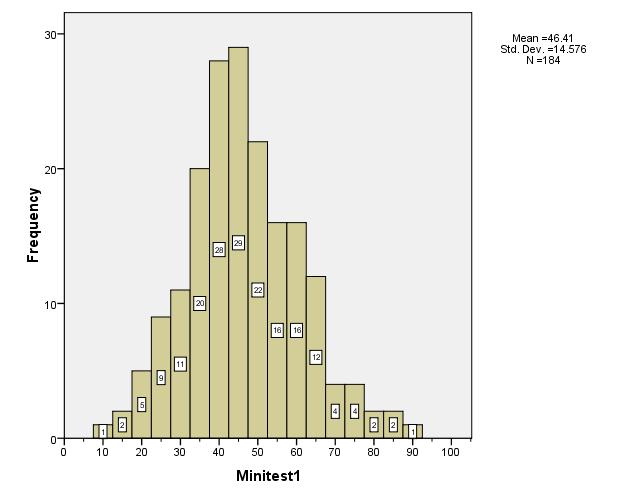
Histogram of the results. Normal distribution.
Individual Results
57.1% failed minitest 1
Histogram of the results. Normal distribution.
Deadline; FK6163 – 15th Oct 2019 at 8am; FF2613 – 25th Oct 2019 at 8am.
How to do the online practical 2
1. Download the practical from HERE. Use these formulas as reference.
2. Do the Practical 2 T-Test on paper first. Get all the answers. Use these notes to help you https://drtamil.me/2013/10/06/ff2613-cl11-t-test/ pw cl12gosset and this Excel file for Q3–prac2-Q3 & Q1&2.
3. Log in into https://docs.google.com/forms/d/10FOv1s-COc6HTRSeaOPf3ZRodlD-t-iIbQcOHX5VUpA/viewform
4. Match the questions on screen to the questions in the practical. Start answering, you have 2 hours to finish the 16 questions. Good luck.
5. This exercise will contribute 2.5 marks to your final marks.
Thank you for your answers. Marks has been posted on your respective FaceBook groups. Here is the video of the answers for the above practical.
Deadline for FK6163 – 3rd Oct 2019 at 8am; FF2613 – 18th Oct 2019 at 8am.
How to do the online practical 1?
1. Download the practical from HERE. Use these formula as reference. You can use ps1-data as a guide.
2. Do the Practical 1 Descriptive Statistics on paper first. Get all the answers. You can refer to the following notes to get the answers; http://www.slideshare.net/drtamil/descriptive-analysis-in-statistics
3. Log in into https://docs.google.com/forms/d/1-Mc6CB1GXqrtWx_z4WtUUJiVpc0lH1GHOwLeuaArYcU/viewform
4. Match the questions on screen to the questions in the practical. Start answering, you have 2 hours to finish the 8 questions. Good luck.
5. This exercise will contribute 2.5 marks to your final marks.
Thank you for your answers. Marks has been posted on your respective FaceBook groups. Here is the video of the answers for the above practical.
Upon graduation, doctors will need to drive a car. It should be reliable enough so that it won’t be breaking down every time you have a medical emergency at the hospital. So should you take the maximum 9-year loan or the shortest 3-year loan?
For a decent local car, we expect the car loan to be around RM64k. At current rates (2.7% for 3 years and 2.6% for 9 years), a three-year loan would have you coughing out MYR1922 per month (about two thirds of your monthly pay) and paying a total of MYR5814 in interest.

3-year loan
A 9-year loan would have you paying MYR732 every month (about a quarter of your monthly pay, therefore less painful) and paying a total of MYR14,976 in interest, about 3 times more compared to the 3-year loan, which is expected since 9 years is 3 times longer than 3 years.
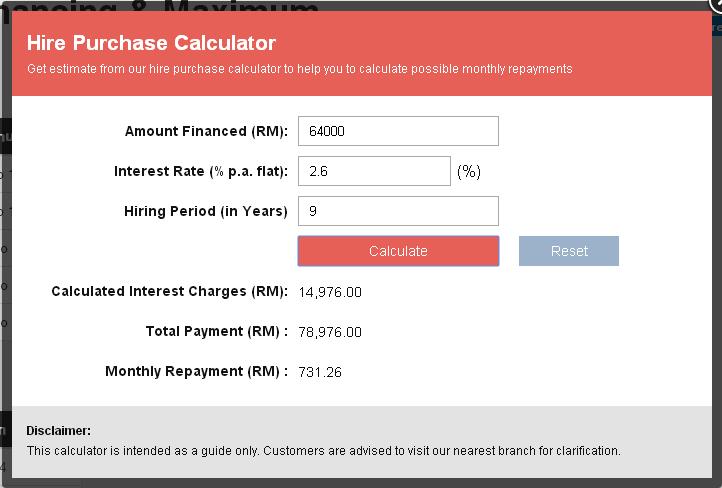
9-year loan
Some would argue that the money saved (MYR1922-MYR732=MYR1190) by taking a longer loan could be invested and that would earn more returns compared to the extra interest paid (MYR14,976-MYR5,814 = MYR9,162).
So let us see if this myth is true? But remember that those in the 3-year loan group can invest the full amount of MYR1922 upon the settlement of their loan. The average dividend rate of Amanah Saham Bumiputera for the last 10 years is 7.5%, which we will use in this calculation.
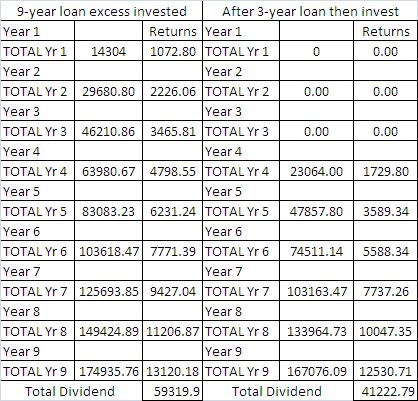
Those who opted for the longer loan ended up with a larger cumulative dividend after 9 years.
You can download the spreadsheet from here.
Those in the 9-year loan group earned more dividend by MYR18,097 and they have a larger amount invested (MYR174,936 versus MYR167,076)
So if you are disciplined enough, you can opt for the longer 9-year loan but you must reinvest the excess amount from the lower monthly installment into your unit trust. Don’t spend it elsewhere. I am a weak man, easily tempted into buying things whenever I have excess cash in hand, so I opted for the shorter 3-year loan.
Disagree? Kindly write-in your feedback in the comments section.
Result of today’s minitest
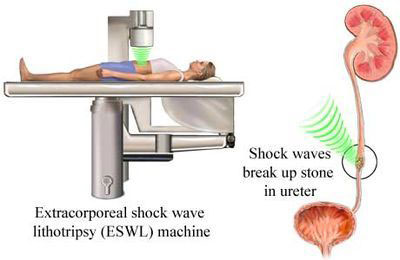
Empathy is the capacity to understand what another person is experiencing from within the other person’s frame of reference, ie, the capacity to place oneself in another’s shoes. Therefore doctors who are able to empathise with their patients, tend to be more compassionate and able to offer better options in treating their patients. If the doctor has experienced the same spectrum of disease as the patient, he would be able to empathise better. When it comes to urolithiasis (stones in the urinary tract), I can empathise very well indeed since I had it 3 times already!
Tersebutlah alkisah……………………
I rode 25km on the trainer on the 8th February 2011. So that night when I suffered acute abdominal pain, I thought it was intestinal obstruction due to old surgical adhesions. It happened once before in November 1993 after shifting house. The increase in exertion caused the scar tissues to strangulate the intestinal loops. Since it was at night, I persevered against the pain and waited for daylight before driving myself to the UKM Hospital. Hoping for the best, I did all the necessary investigation including abdominal X-ray (to look for air/fluid level) and Urine FEME.
Abdominal X-ray 9/2/11
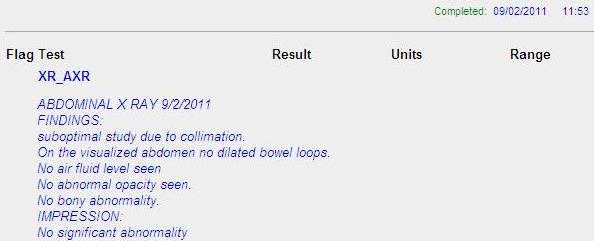
X-ray report
The X-ray report came back as “no abnormalities detected”.

UFEME – RBCs seen in urine.
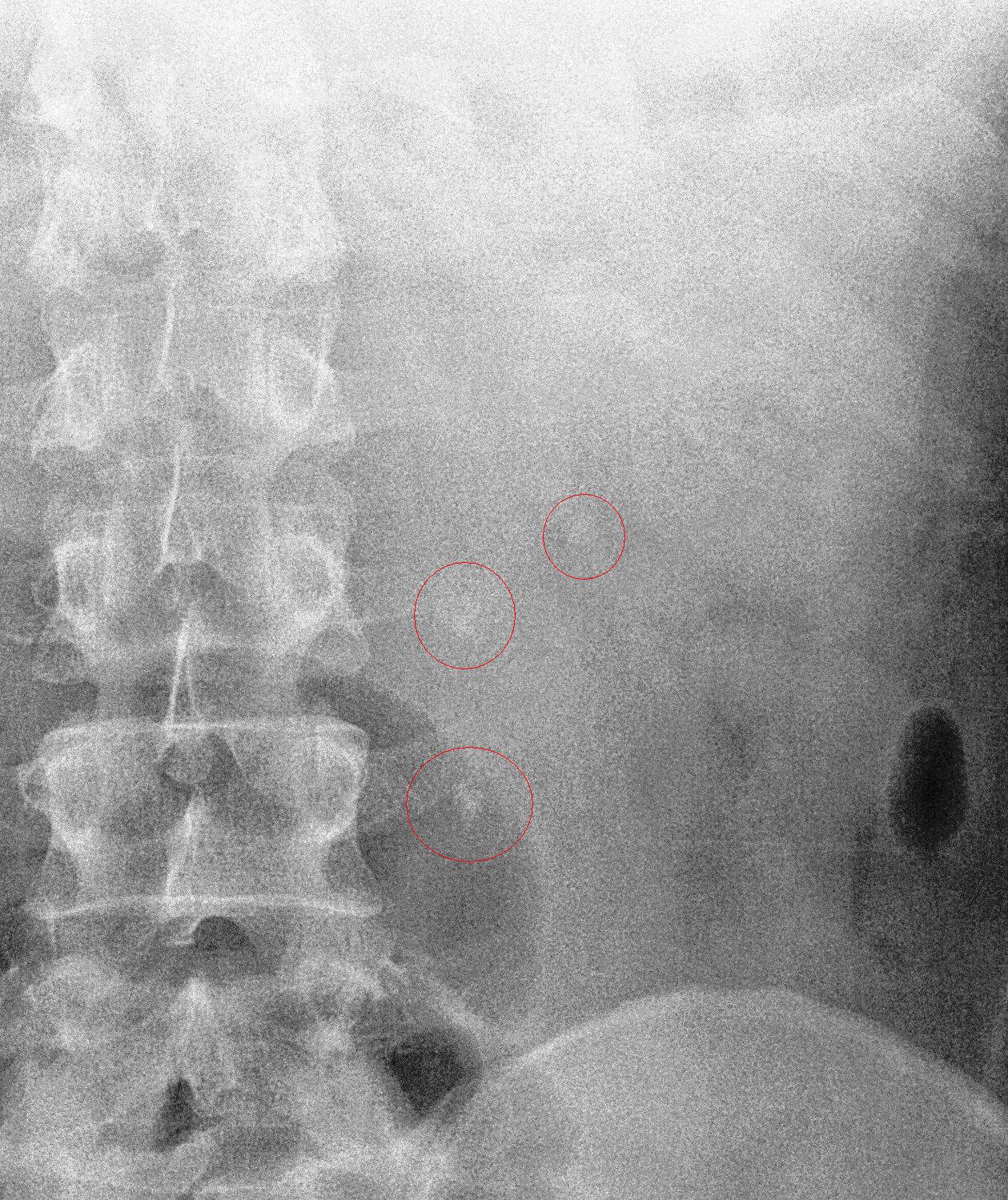
But the Urine FEME came back positive for RBCs, so my provisional diagnosis shifted towards urolithiasis. I downloaded the X-ray film and e-mailed it to a surgeon in Hospital Kuala Lumpur. He confirmed my suspicions by replying, “Congratulations, you got triplets!”.

Location of the 3 stones in reference to the spinal column.
So two days later, I arranged for an ultrasound appointment to confirm the diagnosis of urolithiasis.
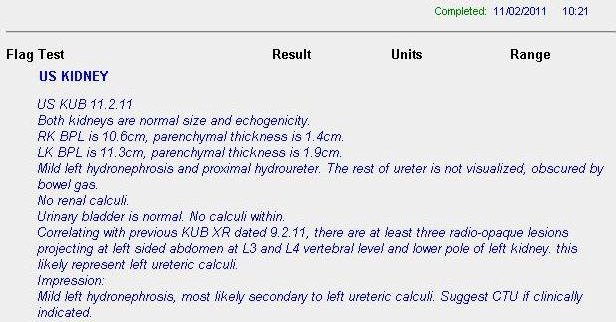
US – confirmation of the urolithiasis.
The ultrasound report confirmed the diagnosis. I started treating myself by ingesting potassium citrate mixture 3 times a day to alkalinise my urine. I also had UFEME done regularly to monitor the presence of RBCs in the urine. A week later on 17th Feb, when the RBCs were no longer being detected in the urine, I had another KUB X-ray done.
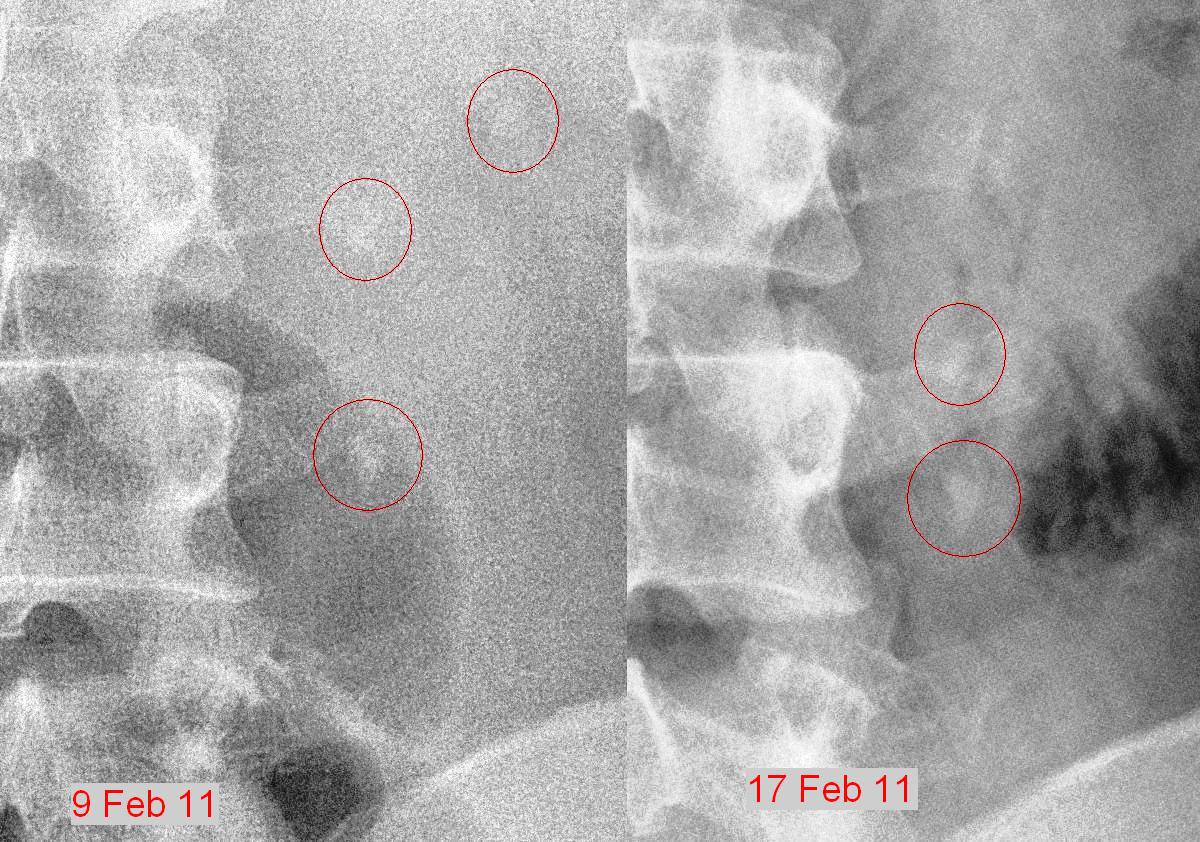
Comparison of the stones location between 9th & 17th Feb.
The KUB on the 17th indicated that the bottom stone was still at the same site but the other two stones has come together and now were on top of each other. But there was no RBCs coming through, so either the bottom stone was blocking everything or the bottom stone had stabilised and was no longer cutting across the surface of my ureter, so no blood in the urine.
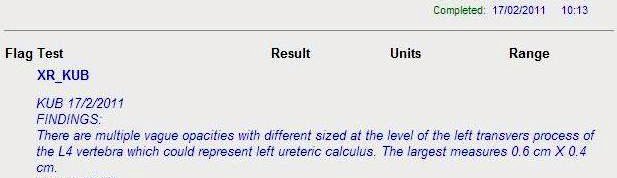
KUB report for 17th Feb.
The uncertainty affected me, since a total blockage would cause a back flow of the urine, thereby affecting my left kidney. I consulted the urologists in UKMMC and they told me to get CT urogram done. I managed to get a CT scan done on the very next day on the 18th Feb.
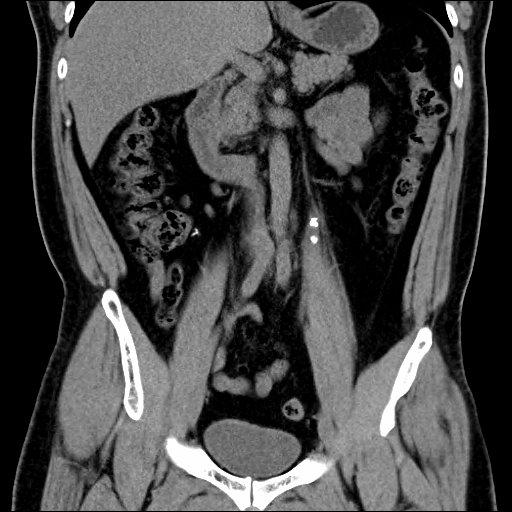
CT Scan showing the location of the 3 stones.
You can clearly see the stones in the CT scan film. Can you see it? Hint – the two white spots in the middle of the picture.
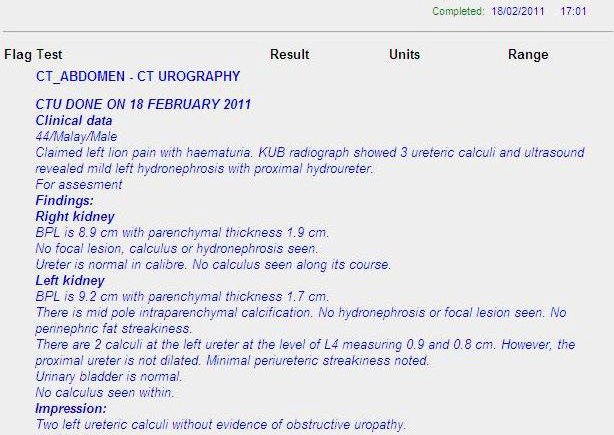
CT Scan report 18 Feb.
The CT scan report indicated that I had 2 humongous stones (9 and 8 mm in diameter). There was no way that these stones could come out through the urethra since they won’t fit through the urethra nor the urethral opening. The UKMMC urologists suggested laser pulverization of the stones and removal via urethroscopy.

Laser pulverisation of the stones.

Removal via urethroscopy.
I readily accepted their suggestion. I was admitted on the 22nd Feb and I was scheduled for surgery at 11 am the next day.

One of the three anesthesiologists in the OT room.
Words travel fast in the OT and suddenly I had 3 anesthesiologists in the room, one a former course mate and the other my cycling buddy. The cycling buddy kindly gave gas via mask throughout the whole procedure, so that when I woke up, there was no throat pain due to the endotracheal tube insertion. Thanks Prof! The procedure took longer than expected since the third stone flew back into the kidney when the second one was being imploded by laser. It was only done by 3 pm. So I really owe all of them a big thanks!

Post-surgery – confirming the location of the stent.
After surgery, there was another KUB done to confirm the location of the stent. The stent protects the ureter from any leftover debris of the pulverised stones.
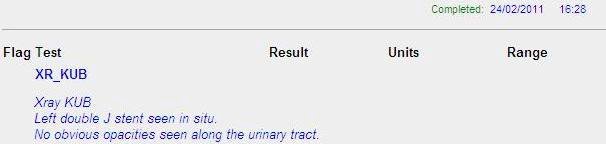
KUB report for 24th Feb.
The X-ray report confirmed that the stent was in the right place. I was out of the OT by 3 pm. At 6pm, the surgeon allowed me to remove the CBD (continuous bladder drainage). I was no longer bed-ridden therefore I was a happy man, and I immediately went down to surau to pray asar and qada’ zohor. Sadly the shops were closed already by then, so I couldn’t buy anything to eat. After 24 hours of observation, I was discharged on Friday morning.
The discharge procedure was tedious, especially the wait at the discharge pharmacy. After more than one hour of waiting, I was only given Panadol for my pain control! Those prescribing did not realise that Arcoxia was not available for discharged patients. I drove myself back to Subang and surprised my wife. She was on the line with my mother, who was telling my wife to go and pick me up at the hospital. But I was already home!
Life with the stent was horrible though. You would be passing urine almost every hour, day and night. As your bladder becomes smaller with micturition, the lower end of the stent would be pulled downwards. Therefore it would also pull down your kidney. That pain had to be experienced to be believed. It was worse than the pain of the stones itself!
After 3 weeks, I had severe pain upon micturition and the stent was removed on 16th March via local anaesthesia. After removal, I passed out blood clots in my urine for a whole day. I didn’t know why the clots were there nor what was causing that intense pain. Anyway I was glad that the stent was gone.

The stent after removal on 16th Feb.
I was on Uracil (potassium citrate mixture) for a few months after that. Hopefully the urolithiasis won’t recur again. My utmost thanks to the Urologist team in UKMMC. I wish I could name all of those who have assisted with my care but it may be a breach of their privacy.
Anyway you know who you are, and thanks bros & sis.
“A friend in need, is a friend indeed!”
Lecture notes – download from HERE;
For the coming SGD session, please critique the following journal;
– Patient Satisfaction toward Medical Ward Services in a Teaching Hospital (TH) And a General Hospital (GH) by USM lecturers.
(Click here to download)
Please use this checklist to critique the above journal.
Click here for another PowerPoint presentation on journal critique.
Extra reading;
CMA Journal Series on “How To Read Clinical Journals”;
1. MMC 2011. HIV & Blood Borne Virus Infections MMC Guidelines
2. Centers For Disease Control 2002. Preventing Occupational HIV Transmission to Healthcare Personnel . CDC HIV/AIDS Prevention. Originally from: http://www.cdc.gov/hiv/resources/factsheets/hcwprev.htm now no longer available.
New updated link:
https://www.cdc.gov/hiv/pdf/library/factsheets/occupational-hiv-transmission-and-prevention-among-healthcare-workers.pdf
3. Centers For Disease Control 2001. Updated U.S. Public Health Service Guidelines for the Management of Occupational Exposures to HBV, HCV, and HIV and Recommendations for Post-exposure Prophylaxis. MMWR June 29, 2001 / 50(RR11);1-42. Originally from: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5011a1.htm
Still available.
4. Centers For Disease Control 1998. Facts about Surveillance of Health Care Workers with HIV/AIDS. CDC HIV/AIDS Prevention. Originally from http://www.cdc.gov/hiv/pubs/facts/hcw98.htm now no longer available.
Newly updated content at;
Centers For Disease Control 2010. Surveillance of Occupationally Acquired HIV/AIDS in Healthcare Personnel, as of December 2010 http://www.cdc.gov/HAI/organisms/hiv/Surveillance-Occupationally-Acquired-HIV-AIDS.html (Still available)
5. Centers for Disease Control 1989. Guidelines for Prevention of Transmission of HIV and Hepatitis B Virus to Health Care & Public-Safety Workers. MMWR 38(S6):1-37.
1989 – Guidelines for Prevention of Transmission of Human Immunodeficiency Virus and Hepatitis B Virus to Health-Care and Public-Safety Workers.txt – Notepad (pdf)
6. Centers for Disease Control 1988. Update: Universal Precautions for Prevention of Transmission of HIV and Hepatitis B Virus and other Bloodborne Pathogens in Health-Care Settings. MMWR 37(24):387-388.
1988-Update Universal Precautions for Prevention of Transmission of Human Immunodeficiency Virus, Hepatitis B Virus, and Other Bloodborne Pathogens in Health-Care Settings.TXT – Notepad (pdf)
7. Centers for Disease Control 1987. Recommendations for prevention of HIV transmission in health-care settings. MMWR 1987;36 (suppl no. 2S) :S1-S18. Originally from http://www.cdc.gov/mmwr/preview/mmwrhtml/00023587.htm (poorly formatted on the web)
1987 – Recommendations for Prevention of HIV Transmission in Health-care Settings – Notepad (pdf).
8. Ministry of Health Malaysia 1995. Guidelines on the Management of Infected Healthcare Workers.
– Partial
– Complete
Please do this practical before coming to class.
Please refer to these NOTES for help with the exercises.
Please submit your answers HERE. Deadline 14th October 2021 8am.

{kind=link}